2016: Creating a Culture of Safety in Oncology
Creating a safe environment is everyone’s job—oncology nurses, managers, administrators, national organizations, and family members and caregivers. Working together, we can create a culture of safety that improves the quality of care for patients with cancer, decreases adverse events for patients and healthcare workers, and integrates a humane system for reporting errors to help identify areas for quality improvement.
Jump to a section
Nurses play vital roles in preventing errors and improving the quality of care for patients. However, in the breakthrough Institute of Medicine (IOM) reports, To Err Is Human: Building a Safer Health System (IOM, 1999) and Crossing the Quality Chasm: A New Health System for the 21st Century (IOM, 2001), it was estimated that about 44,000–98,000 Americans die each year as a result of medical errors. Gibson and Singh’s (2003) book, Wall of Silence: The Untold Story of the Medical Mistakes That Kill and Injure Millions of Americans, shared real-life stories of medical mistakes to help raise awareness and create a sense of urgency for the issues surrounding healthcare errors. Gibson and Singh (2003) also included aspects of the human side of errors—the perceptions of the healthcare providers regarding their errors and the responses of patients who had been harmed.
Many actions to improve the safety of the healthcare environment and reduce adverse events for patients have been taken since the publication of those three reports (Gibson & Singh, 2003; IOM, 1999, 2001). Nurses have been instrumental in many of the initiatives to improve patient safety and the quality of care. For example, in 2011, the American Nurses Association (ANA) partnered with the Centers for Medicare and Medicaid Services (CMS) to form the Partnership for Patients (PfP) (http://1.usa.gov/1oYECMJ). The focus of PfP is quality improvement, patient safety, and cost-effective patient care (CMS, n.d.). The three key elements of this partnership have been widely implemented: hospital engagement networks (currently 17 contracts), community-based care transitions programs (in 46 sites), and patient and family engagement to improve the relationship between healthcare professionals and patients and their families.
A specific initiative of PfP is to reduce hospital-acquired conditions, such as catheter-associated urinary tract infections (CAUTI). In response, the ANA (n.d.) developed the CAUTI prevention tool using an expert panel, evidence, and previously published guidelines from the Centers for Disease Control and Prevention (2009). The tool is a nurse-driven protocol to decrease urinary tract infections in hospitalized patients.
In addition, the ANA has launched the 2016 Culture of Safety campaign (http://bit.ly/1TS0LYd). This year-long campaign is the result of the sustained commitment of organizations, such as the ANA, and leaders, managers, and healthcare workers in clinical care to emphasize safety over competing goals.
Other national organizations are involved in defining the role of healthcare institutions in creating a culture of safety. The Agency for Healthcare Research and Quality (2014) has outlined the key features for establishing a culture of safety:
• Acknowledgment of the high-risk nature of an organization’s activities and the determination to achieve consistently safe operations
• A blame-free environment where individuals are able to report errors or near misses without fear of reprimand or punishment
• Encouragement of collaboration across ranks and disciplines to seek solutions to patient safety problems
• Organizational commitment of resources to address safety concerns.
Across healthcare organizations, settings, and professions, there has been an impetus to share evidence from research and practice settings and improve reporting of errors and near misses to enhance safety in health care (Leonard, Frankel, Federico, Frush, & Haraden, 2013) (see Figure 1).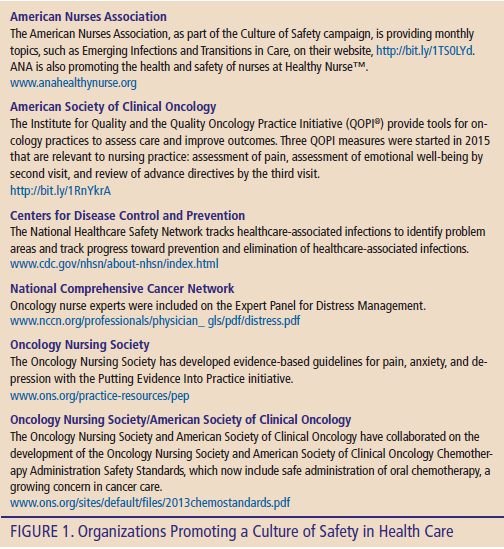
Cancer care is complex and sometimes hazardous work that requires extra vigilance to maintain safety in care delivery for patients and providers. Oncology nurses work hard to increase the quality of care from chemotherapy and radiation therapy delivery to minimize adverse events for patients. Oncology nurses also understand that a blame-free environment is needed so that clinicians report errors or near misses to help identify problem areas and adjust and improve care-delivery systems.
The Clinical Journal of Oncology Nursing has historically addressed the issues of safety with two key columns: Safety, which debuted in 2008, and Quality, which debuted in 2013.
The Safety column, edited by associate editor David Glenn, RN, MS, examines potential hazards such as medications, falls, radiation risks, oncologic emergencies, and other safety concerns that may affect patients with cancer and the nurses and family caregivers who care for them. The Quality column, edited by associate editor Anne Gross, PhD, RN, FAAN, disseminates quality improvement work in oncology care that has improved cancer care. More information about these two columns can be found at https://cjon.ons.org/content/columns-and-editorial-board.
Creating a safe environment is everyone’s job—oncology nurses, managers, administrators, national organizations, and family members and caregivers. Working together, we can create a culture of safety that improves the quality of care for patients with cancer, decreases adverse events for patients and healthcare workers, and integrates a humane system for reporting errors to help identify areas for quality improvement.
References
Agency for Healthcare Research and Quality. (2014). Safety culture. Retrieved from https://psnet.ahrq.gov/primers/primer/5/safety-culture
American Nurses Association. (n.d.). ANA CAUTI prevention tool. Retrieved from http://nursingworld.org/ANA-CAUTI-Prevention-Tool
Centers for Disease Control and Prevention. (2009). Guideline for prevention of catheter-associated urinary tract infections, 2009. Retrieved from http://www.cdc.gov/hicpac/cauti/001_cauti.html
Centers for Medicare and Medicaid Services. (n.d.). About the Partnership for Patients. Retrieved from http://1.usa.gov/1oYECMJ
Gibson, R., & Singh, J.P. (2003). Wall of silence: The untold story of the medical mistakes that kill and injure millions of Americans. Jackson, TN: Perseus Distribution Services.
Institute of Medicine. (1999). To err is human: Building a safer health system. Washington, DC: National Academies Press.
Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press.
Leonard, M., Frankel, A., Federico, F., Frush, K., & Haraden, C. (Eds.). (2013). The essential guide for patient safety officers (2nd ed.). Oakbrook Terrace, IL: Joint Commission Resources.
About the Author(s)
Lisa Kennedy Sheldon, PhD, APRN, BC, AOCNP®, is an associate professor in the College of Nursing and Health Sciences at the University of Massachusetts–Boston and an oncology nurse practitioner in the Cancer Center at St. Joseph Hospital in Nashua, NH. The author takes full responsibility for the content of the article. No financial relationships relevant to the content of this article have been disclosed by the editorial staff. Kennedy Sheldon can be reached at CJONEditor@ons.org.


