Nurse-Led Supportive Care Intervention for Men With Advanced Prostate Cancer: Healthcare Professionals' Perspectives
Purpose: To identify barriers and corresponding solutions for implementing a telephone-based, nurse-led supportive care intervention for men with advanced prostate cancer.
Participants & Setting: 21 healthcare professionals with an average 15.81 years of experience in diverse prostate cancer care settings.
Methodologic Approach: Data from semistructured interviews were coded into the Theoretical Domains Framework and mapped to behavior change techniques (BCTs) to inform the development of an implementation schema.
Findings: Barriers included lack of knowledge about the effectiveness of survivorship interventions and how to deliver them, low referral rates to psychosocial oncology care, low help-seeking behavior among men with advanced prostate cancer, lack of care coordination skills, and inadequate service capacity.
Implications for Nursing: Interprofessional support exists for a nurse-led supportive care intervention. Causes of low engagement with supportive care among men with advanced prostate cancer extend beyond gendered patterns of response.
Jump to a section
Prostate cancer survivorship interventions are delivered from diagnosis to death and can alleviate the physical symptoms of cancer (Beaudry et al., 2018), reduce cancer-related distress, and enhance health-related quality of life (Chambers, Ng, et al., 2017). Broadly, prostate cancer survivorship interventions have four essential components: prevention, surveillance, intervention, and coordination for men living with prostate cancer and their partners (Hewitt, Greenfield, & Stovall, 2006). However, the scope and number of available survivorship interventions for men living with prostate cancer are limited. In a systematic review by Crawford-Williams et al. (2018) of interventions targeting the five domain areas of the American Cancer Society’s prostate cancer survivorship care guidelines (Skolarus et al., 2014), effective interventions were found for health promotion, physical side effects, and psychosocial management, although none were identified for improving surveillance or care coordination. Developing and implementing additional survivorship interventions is necessary to advance survivorship care and improve outcomes among survivors and their loved ones. However, intervention development is fraught with risk; many fail because of their clinical ineffectiveness, low uptake among healthcare professionals, or both (Alonso-Coello et al., 2010; Pollack, Hawkins, Peaker, Buchanan, & Risendal, 2011). Causes of failure are complex and often linked with factors beyond the intervention design, such as poor survivor engagement, limitations in technologic support, a lack of awareness or skill among healthcare professionals, low clinician support, resource limitations, challenging regulatory environments, and poorly implemented interventions (Pollack et al., 2011).
Implementing effective survivorship interventions is vital, because unmet needs among prostate cancer survivors remain high over time. An Australian study by Steginga et al. (2001) reported that as many as 33% of men have moderate to high needs. Another Australian study by Smith et al. (2007) indicated that 54% of men have unmet needs. A systematic review by Paterson, Robertson, Smith, and Nabi (2015) showed high unmet needs in men related to intimacy (65%), information (77%), physical symptoms (47%), and psychological distress (53%) worldwide.
For men with advanced disease, additional physical and psychological challenges can stem from treatment-related side effects from hormonal ablation, the main treatment for advanced disease, including mood disturbance, sarcopenia, increased fat mass, cognitive decline, fatigue, and sexual dysfunction (Australian Cancer Network Management of Metastatic Prostate Cancer Working Party, 2010). Compared to men with localized prostate cancer, men with advanced disease report higher levels of psychological distress and poorer quality of life (Bloch et al., 2007; Eton & Lepore, 2002). In addition, men with advanced prostate cancer have an increased risk of suicide compared to men with localized disease, and rural men have lower survival rates (Bill-Axelson et al., 2010; Dasgupta et al., 2019). Unmet psychological supportive care needs are highly prevalent in men with advanced prostate cancer, with more than half (54%) reporting unmet psychological needs (Smith et al., 2007). One in four men with advanced disease has a moderate to high need for help with feeling uncertain about the future, and one in five reports a moderate to high need for help with feeling anxious (Smith et al., 2007). About one in four men experiences regret about treatment decisions, which is associated with poorer quality of life and increased distress (Clark, Wray, & Ashton, 2001).
Emotional distress can predict further health deterioration (Punnen et al., 2013), with one study reporting a link between heightened psychological distress and declining physical health among men with advanced disease, including urinary, bowel, and sexual dysfunction (Orom, Biddle, Underwood, & Nelson, 2018). These data show that men living with prostate cancer face a sustained and varied burden of disease, highlighting the need for supportive care interventions that treat physical, psychological, and social symptoms.
Purpose
In a climate marked by sustained and extensive unmet needs, healthcare professionals must be equipped with effective supportive care interventions to care for men with advanced prostate cancer. However, several studies have reported concerns among healthcare professionals about the effectiveness and feasibility of interventions, such as support groups and survivorship care plans, leading to low referral rates (Oliffe et al., 2015; Steginga et al., 2007). In addition, barriers to sustaining and scaling these survivorship interventions include a lack of empirical program evaluations, unwillingness to refer, limited resources (Gosselin, Crane-Okada, Irwin, Tringali, & Wenzel, 2011), and lack of knowledge (Luxford, Hill, & Bell, 2006) and organizational support (Botti et al., 2006). Therefore, the authors interviewed healthcare professionals to identify barriers to implementing supportive care for men with prostate cancer and inform the creation of a preimplementation plan for a nurse-led supportive care intervention for men with advanced prostate cancer called ProsCare, which has been reported elsewhere (Ralph, Chambers, Pomery, Ollife, & Dunn, 2019) and is outlined in Figure 1. 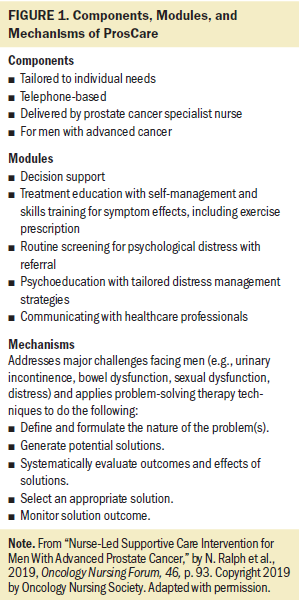
Participants and Setting
This study was approved by the Griffith University Human Research Ethics Committee (HREC 2017/628). The authors conducted individual interviews with 21 Australian healthcare professionals working in prostate cancer care (7 RNs, 4 radiation oncologists, 3 urologists, 3 general practitioners, 1 medical oncologist, 1 psychologist, 1 physiotherapist, and 1 exercise physiologist). The mean age of participants was 53.52 years (SD = 8.42). Twelve participants were men, and nine were women. Participants’ mean practice experience was 25.48 years (SD = 10.11); their mean advanced prostate cancer experience was 15.81 years (SD = 9.49). Participants were contacted via a mailing list through the Australian National Health and Medical Research Council’s Centre for Research Excellence in Prostate Cancer Survivorship, and those expressing an interest in participating were consented. To be eligible, all participants were required to have more than five years of experience working in prostate cancer care and a role reflective of extensive expertise (e.g., consultant medical or surgical specialist, nurse specialist, senior allied health manager). Informed consent was obtained from all individuals included in the study. Quasi-structured interviews were conducted (time range = 20 minutes to an hour), transcribed verbatim, checked for accuracy, and coded within NVivo. Participants were asked to describe the implementation climate for supportive care interventions, including barriers and enablers, men’s engagement with supportive care interventions, and perspectives on supportive care interventions (i.e., ProsCare).
Ethical Approval
All procedures involving human participants were performed in accordance with the ethical standards of the Griffith University HREC and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Data were consecutively and independently coded by two authors into a framework and were adjudged as being theoretically saturated using criteria established by Glaser and Strauss (2017) (Ralph, Birks, & Chapman, 2015). As used by French et al. (2012), the current authors adapted a stepped approach to direct data collection and analysis in which guiding questions informed the investigation of how to optimize processes of implementation.
Methodologic Approach
Step 1: Who Needs to Do What Differently?
Realist evaluation theory was used to investigate what works, in which circumstances, and for whom (Pawson & Tilley, 1997). The authors questioned participants on issues relating to an interventional schema that they concomitantly developed in another study (Ralph et al., 2019). The authors probed for data on interventional need, intervention delivery, and barriers to implementation by asking the following:
• What are the challenges that men with advanced prostate cancer face?
• What supports are available to men with advanced prostate cancer?
• How do healthcare professionals and men with advanced prostate cancer perceive psychosocial care?
• What contexts (e.g., geography) may influence the uptake of psychosocial interventions by men with prostate cancer or their use among healthcare professionals?
Prompting was used to encourage participants to expand on behavior-related barriers that affected the effectiveness or uptake of supportive care among men with advanced prostate cancer, who engages in these behaviors, and where and when these behaviors occur.
Step 2: Which Barriers and Enablers Need to Be Addressed?
The authors chose the Theoretical Domains Framework (TDF) because it uses an evidence-based schema, derived from theory, for identifying determinants of behavior (Atkins et al., 2017; Michie, Johnston, Francis, Hardeman, & Eccles, 2008). The TDF contains 14 domains and associated characteristics, which can overlap and interrelate (see Table 1). These domains provide a way to categorize positive and negative influences on program implementation and opportunities to strengthen intervention design and process implementation (Atkins et al., 2017). 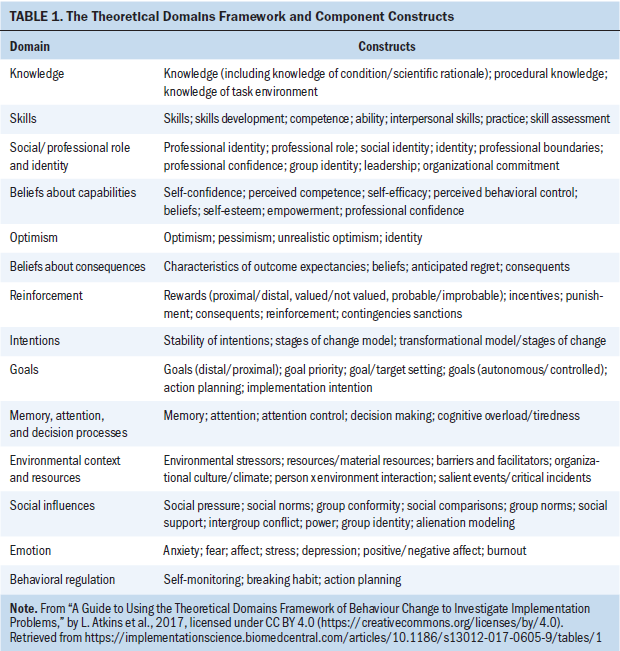
Step 3: Which Intervention Components Could Overcome the Modifiable Barriers and Enhance the Enablers?
As outlined by Michie et al. (2008), two authors collaboratively identified behavior change techniques (BCTs) to mitigate barriers and strengthen enablers related to implementation. Barriers to implementation were iteratively coded and refined until two authors agreed on their representativeness. BCTs were then mapped to the barriers identified in each TDF domain. The BCTs selected were chosen based on what the authors adjudged to be most suitable to the context and most likely to be feasible and ideal for scaling. Tested interventions aligned to the BCTs were then identified in the literature and mapped to reflect realist theory’s context–mechanism–outcome algorithm of implementation (Pawson & Tilley, 1997). The authors augmented the process used by French et al. (2012) by systematically searching CINAHL®, PubMed, PsycINFO, Cochrane Database of Systematic Reviews, and Scopus for evidence on modes of delivery for behavior change. The authors used permutations of the following search terms: target behaviour, implementation intervention, behaviour change technique, and modifiable barrier. English articles dating back to 2000 and relevant to addressing barriers and enablers were selected by two reviewers (N.R. and K.L.) and referenced in findings using consensus. For example, low awareness of supportive care was an identified barrier; therefore, the authors mapped this to the TDF domain of knowledge and used the mapping table outlined in Michie et al. (2008) to the BCT of information provision, where interventions for providing information are referenced from a Cochrane Review (Forsetlund et al., 2009).
Findings
Data were coded into the TDF, and findings are described with illustrative quotes in Figure 2. 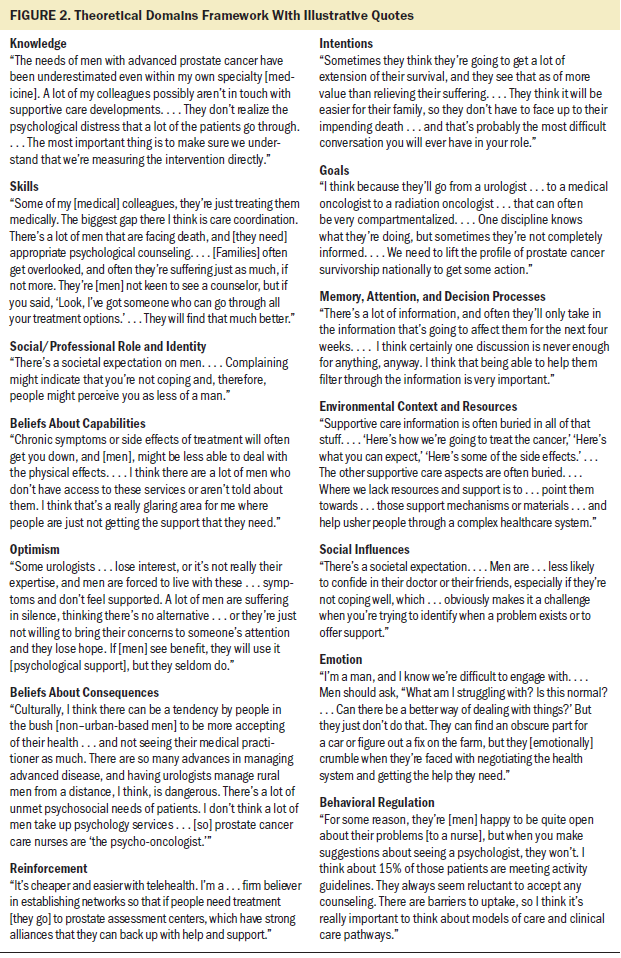
Domain 1: Knowledge
The participants believed that treatment options for men were progressing so quickly that maintaining currency of prostate cancer knowledge was challenging for healthcare professionals. A lack of current psycho-oncologic knowledge was acknowledged, particularly among medical professionals, resulting in variances in assessment of the needs of men with advanced prostate cancer. Healthcare professionals were uncertain about the type of men who benefit from supportive care, with their judgments based on how different personality types may respond to supportive care and social and partner supports. Uncertainty was further compounded by doubts among clinicians about the effectiveness of survivorship interventions; insufficient feedback from previous survivorship initiatives, resulting in a lack of procedural knowledge; and failure to ask men whether they found benefit in supportive care interventions to gain knowledge about their condition.
Domain 2: Skills
Healthcare professionals broadly agreed about the need to develop skills in providing psychological support and coping strategies for men, increasing partner involvement in care, and improving care coordination. Participants, including doctors, expressed a desire for specialists to develop skills in supportive care. There was also broad support for skills development around incorporating partners and family in care and helping them navigate through the system effectively.
Domain 3: Social/Professional Role and Identity
Social norms and identities were addressed by participants because they were seen to influence the uptake of supportive care among men with advanced prostate cancer. Participants expressed concern that stoicism and being a patriarch were common in men, as was low uptake of supportive care. These issues were amplified by the impact of anticancer treatments on masculine identity; mood and the emotions of men profoundly affected their self-concept and reduced their inclination to access treatment.
Domain 4: Beliefs About Capabilities
Participants expressed the belief that men often lacked the competence to cope with a diagnosis of advanced prostate cancer, which was exacerbated by inadequate capabilities in knowing how to access and navigate the healthcare system. Even when men accessed health care, concerns were expressed that the system did not provide adequate services to men with advanced prostate cancer, particularly for psychosocial care.
Domain 5: Optimism
Participants expressed pessimism around the potential for specialists to engage with and refer to supportive care interventions. However, participants also expressed pessimism about the perceived effectiveness of supportive care interventions, which was compounded by a lack of awareness among men about the services available.
Domain 6: Beliefs About Consequences
Participants suggested that the consequences of being stoic strongly contributed to men accepting their fate following a diagnosis of advanced prostate cancer. In turn, this muted men’s likelihood of expressing preferences for additional treatment or care. When medical specialists did not provide or promote psycho-oncologic care or refer to psychology services, nurses working in advanced prostate cancer care were seen to address unmet needs.
Domain 7: Reinforcement
Participants agreed that establishing different models of care was necessary to reinforce efforts for improving the care of men with advanced prostate cancer. Proposals, such as using telehealth to deliver supportive care and a national network of prostate cancer centers, were suggested to increase access to initial and ongoing treatment.
Domain 8: Intentions
Participants believed that men with advanced prostate cancer intended to extend their life more than improve the quality of it, resulting in healthcare professionals being less likely to refer to supportive care services. Although healthcare professionals intended to involve family members, they were often unsure of how to meaningfully include them in changing the emphasis of care.
Domain 9: Goals
The shared goal of participants was to see improved access to psycho-oncologic services for men with prostate cancer, particularly in rural Australia. Participants called for decentralizing access to treatment from hospitals to a model involving “drop-in centers” for improving care coordination. Identifying new models for coordinating care for men with prostate cancer was a shared priority. This included finding ways to engage men in conversations about their care and encourage them to accept help, such as support groups or exercise programs. Therefore, participants shared the goal of developing a public health campaign for prostate cancer to raise awareness and reduce social stigma around the disease.
Domain 10: Memory, Attention, and Decision Processes
Participants reported that memory and decision-making processes were relevant factors for men after a prostate cancer diagnosis. Because men with prostate cancer can struggle with information recall and informed decision making, there was concern that decisions were not revisited and that information initially provided to men may not continue to be relevant when the disease progressed. Some participants valued decision aids, but they were often not provided to men.
Domain 11: Environmental Context and Resources
The challenges of delivering supportive care to men with advanced prostate cancer were addressed by participants, including cost, time, and difficulty accessing services. Participants linked these barriers to limited general awareness about supportive care referral pathways and services among men and general practitioners, particularly in rural Australia. Participants argued for a range of strategies to increase awareness of prostate cancer survivorship challenges and services for them as a way of increasing professional referral and survivor uptake. However, resources were acknowledged as scarce, with relatively few services, such as prostate cancer specialist nurses, available in Australia.
Domain 12: Social Influences
Because of social norms, participants reported that social pressure often caused men to not seek support. Men were also reported to be less likely to reveal psychological distress and seek help from healthcare professionals.
Domain 13: Emotion
Emotion was a factor in participants calling for improved psychosocial care. Following a diagnosis of prostate cancer, men had to deal with the fear, stress, and anxiety of facing death or disease. Their mental status was further compounded by a lack of awareness about the impact that prostate cancer symptoms and treatment side effects had on their psychosocial well-being, as well as stress from being faced with navigating the healthcare system.
Domain 14: Behavioral Regulation
Without emphasized supportive care for men with prostate cancer, breaking habits, such as sedentary lifestyles and poor diet, was seen to be challenging. When partners were not engaged in action planning, healthcare professionals were not fully aware of men’s need for psycho-oncologic care. Participants frequently referred to examples of men preferring to discuss their needs with RNs while avoiding exercise physiologists and refusing referrals to a psychologist because of their associating the need for psychological care with mental illness. Participants saw new models of care and referral pathways as solutions for enabling improved behavioral regulation among men with prostate cancer. Following this analysis, the authors linked these barriers to corresponding BCTs and their modes of delivery (see Table 2). 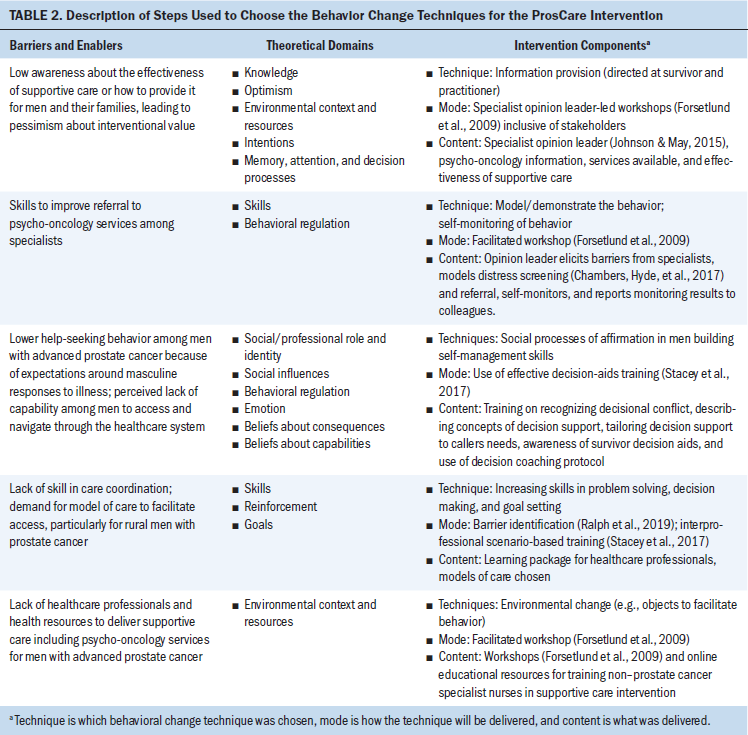
Discussion
The current study extends previous research on the implementation of a supportive care intervention for men with advanced prostate cancer (Ralph et al., 2019) by creating a framework to address barriers using BCTs. Adapting French et al.’s (2012) approach enabled the rigorous selection of strategies that the authors had not previously identified for facilitating the rollout of a supportive care intervention. With more than half of prostate cancer survivors reporting high unmet supportive care needs (Smith et al., 2007), interventional development must include consideration of effectiveness, feasibility, and user friendliness to promote uptake and adherence. Therefore, more work is needed to identify drivers of healthcare access and treatment adherence in men because they typically underuse psycho-oncology care after a cancer diagnosis. However, discordantly, these men report significant unmet needs, including fatigue, cognitive function, and sarcopenia, often as a result of androgen deprivation therapy (Chambers et al., 2018). An Australian study by Chambers et al. (2018) of 32 men with advanced prostate cancer reported that men felt distressed about late diagnosis and treatment decisions, being discounted in the healthcare system, fear/uncertainty about the future, acceptance of their situation, masculinity, and treatment effects. Despite the need to address unmet needs, resourcing of psycho-oncology services is problematic because of reported gaps between the breadth of need and the availability of effective and easily deployable solutions (Ralph et al., 2019). To bridge these gaps, further research is needed to identify effective ways to treat a vast number of men and their loved ones in resource-limited contexts.
Therefore, the authors argue for a system-wide approach that promotes the value and urgency of targeted psychosocial care for men with advanced prostate cancer. This approach should acknowledge masculine models of coping and establish a context wherein men are expected, encouraged, and affirmed to use healthcare services and access support in the broader community—akin to widespread social expectations around adherence to biomedical services. The participants’ testimonies reflected significant challenges in care provision, with barriers to uptake more frequently seen as organizational or systemic issues in the current study findings than nuanced complexities regarding men’s reticence for help seeking. The current study highlights the importance of reframing models of care to be more “man-friendly” and cognizant of masculine models of coping and how men respond to a diagnosis of prostate cancer.
Strengths and Limitations
The study is limited by participants being healthcare professionals within Australia; therefore, consideration was given to an implementation climate-reflective of the Australian healthcare system. Although the authors’ approach to preimplementation planning is useful for using expert healthcare professionals to inform barrier identification and for responding to these barriers with targeted and theory-based solutions (Finnell, Stanton, & Downs, 2014), a limitation of this approach is that the effect of educational strategies on changes to implementation uptake are poorly understood, with further research needed in the area (Forsetlund et al., 2009; Grudniewicz et al., 2015). Study strengths include a highly experienced and broad sample of healthcare professionals working in prostate cancer survivorship care for an average of more than 15 years. As a limitation, being a study of Australian healthcare professionals, the findings may not be transferable to dissimilar populations and cultures and may not apply to low and middle-income countries. 
Implications for Nursing and Conclusion
The findings have broad application to stakeholders aiming to identify evidence-informed methods for the prospects of a successful implementation. Although this study is specifically focused on a nurse-led intervention for men with advanced prostate cancer, it is broadly applicable to clinicians and researchers working to develop survivorship interventions in cancer care because the barriers faced are similar. Given the challenges of implementation reported in the literature, identifying solutions to lower the chance of failure is fundamental to addressing unmet needs among cancer survivors. Identifying barriers using a valid implementation framework and posing solutions to each of these issues using theory is a valuable approach for improving readiness for implementation. If adopted, these findings will significantly extend the supports available to improving the design and implementation of ProsCare. It will also facilitate careful and detailed expansion based on the latest evidence, contexts of care, implementation strategies, and behavioral change strategies to minimize the risk of nonadoption. With emerging preimplementation methods, it is necessary to report the effect of behavioral change strategies implementation success. Outcomes for measuring success may include use of distress screening and referral to and uptake of psycho-oncologic services among men with prostate cancer. [[{"fid":"54361","view_mode":"default","fields":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false},"link_text":null,"type":"media","field_deltas":{"1":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false}},"attributes":{"class":"media-element file-default","data-delta":"1"}}]]
The authors gratefully acknowledge Jaycie Bohan, BPsych, for research assistance.
About the Author(s)
Nicholas Ralph, PhD, BN, RN, is an associate professor in the School of Nursing and Midwifery at the University of Southern Queensland and a senior manager in Health Systems and Psycho-Oncology at the Cancer Council Queensland in Brisbane, Suzanne K. Chambers, PhD, RN, is the dean of the Faculty of Health at the University of Technology Sydney, and Kirstyn Laurie, BPsych(Hons), is a research officer in the Cancer Research Centre at Cancer Council Queensland in Brisbane, all in Australia; John Oliffe, PhD, MEd, RN, is a professor in the School of Nursing and Midwifery at the University of British Columbia in Vancouver, Canada; Mark Lazenby, PhD, APRN, FAPOS, FAAN, is a professor in the School of Nursing at the University of Connecticut in Storrs; and Jeff Dunn, PhD, is the chief executive officer of the Prostate Cancer Foundation of Australia in Sydney, New South Wales, and a professor in the Research and Innovation Division at the University of Southern Queensland Springfield. This research was funded by the Prostate Cancer Foundation of Australia and University of Southern Queensland “Surviving Prostate Cancer in Regional Australia” project and the National Health and Medical Research Council Centre for Research Excellence in Prostate Cancer Survivorship (APP1098042). Ralph, Chambers, Lazenby, and Dunn contributed to the conceptualization and design. Chambers, Laurie, and Dunn competed the data collection. Ralph, Chambers, Laurie, Oliffe, and Dunn provided analysis. All authors contributed to the manuscript preparation. Ralph can be reached at nicholas.ralph@usq.edu.au, with copy to ONFEditor@ons.org. (Submitted February 2019. Accepted July 11, 2019.)
References
Alonso-Coello, P., Irfan, A., Solà, I., Gich, I., Delgado-Noguera, M., Rigau, D., . . . Schunemann, H. (2010). The quality of clinical practice guidelines over the last two decades: A systematic review of guideline appraisal studies. Quality and Safety in Health Care, 19, e58. https://doi.org/10.1136/qshc.2010.042077
Atkins, L., Francis, J., Islam, R., O’Connor, D., Patey, A., Ivers, N., . . . Michie, S. (2017). A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science, 12, 77. https://doi.org/10.1186/s13012-017-0605-9
Australian Cancer Network Management of Metastatic Prostate Cancer Working Party. (2010). Clinical practice guidelines for the management of locally advanced and metastatic prostate cancer. Sydney, Australia: Cancer Council Australia and Australian Cancer Network. Retrieved from https://www.cancer.org.au/content/pdf/HealthProfessionals/ClinicalGuide…
Beaudry, R.I., Liang, Y., Boyton, S.T., Tucker, W.J., Brothers, R.M., Daniel, K.M., . . . Haykowsky, M.J. (2018). Meta-analysis of exercise training on vascular endothelial function in cancer survivors. Integrative Cancer Therapies, 17, 192–199. https://doi.org/10.1177/1534735418756193
Bill-Axelson, A., Garmo, H., Lambe, M., Bratt, O., Adolfsson, J., Nyberg, U., . . . Stattin, P. (2010). Suicide risk in men with prostate-specific antigen–detected early prostate cancer: A nationwide population-based cohort study from PCBaSe Sweden. European Urology, 57, 390–395. https://doi.org/10.1016/j.eururo.2009.10.035
Bloch, S., Love, A., Macvean, M., Duchesne, G., Couper, J., & Kissane, D. (2007). Psychological adjustment of men with prostate cancer: A review of the literature. BioPsychoSocial Medicine, 1, 2. https://doi.org/10.1186/1751-0759-1-2
Botti, M., Endacott, R., Watts, R., Cairns, J., Lewis, K., & Kenny, A. (2006). Barriers in providing psychosocial support for patients with cancer. Cancer Nursing, 29, 309–316. https://doi.org/10.1097/00002820-200607000-00010
Chambers, S.K., Hyde, M.K., Laurie, K., Legg, M., Frydenberg, M., Davis, I.D., . . . Dunn, J. (2018). Experiences of Australian men diagnosed with advanced prostate cancer: A qualitative study. BMJ Open, 8(2), e019917. https://doi.org/10.1136/bmjopen-2017-019917
Chambers, S.K., Hyde, M.K., Smith, D.P., Hughes, S., Yuill, S., Egger, S., . . . Dunn, J. (2017). New challenges in psycho-oncology research III: A systematic review of psychological interventions for prostate cancer survivors and their partners: Clinical and research implications. Psycho-Oncology, 26, 873–913. https://doi.org/10.1002/pon.4431
Chambers, S.K., Ng, S.K., Baade, P., Aitken, J.F., Hyde, M.K., Wittert, G., . . . Dunn, J. (2017). Trajectories of quality of life, life satisfaction, and psychological adjustment after prostate cancer. Psycho-Oncology, 26, 1576–1585. https://doi.org/10.1002/pon.4342
Clark, J.A., Wray, N.P., & Ashton, C.M. (2001). Living with treatment decisions: Regrets and quality of life among men treated for metastatic prostate cancer. Journal of Clinical Oncology, 19, 72–80. https://doi.org/10.1200/JCO.2001.19.1.72
Crawford-Williams, F., March, S., Goodwin, B.C., Ralph, N., Galvão, D.A., Newton, R.U., . . . Dunn, J. (2018). Interventions for prostate cancer survivorship: A systematic review of reviews. Psycho-Oncology, 27, 2339–2348. https://doi.org/10.1002/pon.4888
Dasgupta, P., Baade, P.D., Aitken, J.F., Ralph, N., Chambers, S.K., & Dunn, J. (2019). Geographical variations in prostate cancer outcomes: A systematic review of international evidence. Frontiers in Oncology, 9, 238. https://doi.org/10.3389/fonc.2019.00238
Eton, D.T., & Lepore, S.J. (2002). Prostate cancer and health-related quality of life: A review of the literature. Psycho-Oncology, 11, 307–326. https://doi.org/10.1002/pon.572
Finnell, S.M., Stanton, J.L., & Downs, S.M. (2014). Actionable recommendations in the Bright Futures child health supervision guidelines. Applied Clinical Informatics, 5, 651–659. https://doi.org/10.4338/ACI-2014-02-RA-0012
Forsetlund, L., Bjørndal, A., Rashidian, A., Jamtvedt, G., O’Brien, M.A., Wolf, F., . . . Oxman, A.D. (2009). Continuing education meetings and workshops: Effects on professional practice and health care outcomes. Cochrane Database Systematic Reviews, 2009(2), Cd003030. https://doi.org/10.1002/14651858.CD003030.pub2
French, S.D., Green, S.E., O’Connor, D.A., McKenzie, J.E., Francis, J.J., Michie, S., . . . Grimshaw, J.M. (2012). Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the Theoretical Domains Framework. Implementation Science, 7, 38. https://doi.org/10.1186/1748-5908-7-38
Glaser, B.G., & Strauss, A.L. (2017). The discovery of grounded theory: Strategies for qualitative research. New York, NY: Routledge.
Gosselin, T.K., Crane-Okada, R., Irwin, M., Tringali, C., & Wenzel, J. (2011). Measuring oncology nurses’ psychosocial care practices and needs: Results of an Oncology Nursing Society psychosocial survey. Oncology Nursing Forum, 38, 729–737. https://doi.org/10.1188/11.ONF.729-737
Grudniewicz, A., Kealy, R., Rodseth, R.N., Hamid, J., Rudoler, D., & Straus, S.E. (2015). What is the effectiveness of printed educational materials on primary care physician knowledge, behaviour, and patient outcomes: A systematic review and meta-analyses. Implementation Science, 10, 164. https://doi.org/10.1186/s13012-015-0347-5
Hewitt, M., Greenfield, S., & Stovall, E. (Eds.) (2006). From cancer patient to cancer survivor: Lost in transition. Washington, DC: National Academies Press. https://doi.org/10.21873/anticanres.11960
Johnson, M.J., & May, C.R. (2015). Promoting professional behaviour change in healthcare: What interventions work, and why? A theory-led overview of systematic reviews. BMJ Open, 5(9), e008592. https://doi.org/10.1136/bmjopen-2015-008592
Luxford, K., Hill, D., & Bell, R. (2006). Promoting the implementation of best-practice guidelines using a matrix tool. Disease Management and Health Outcomes, 14, 85–90. https://doi.org/10.2165/00115677-200614020-00003
Michie, S., Johnston, M., Francis, J., Hardeman, W., & Eccles, M. (2008). From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour change techniques. Applied Psychology, 57, 660–680. https://doi.org/10.1111/j.1464-0597.2008.00341.x
Oliffe, J.L., Chambers, S., Garrett, B., Bottorff, J.L., McKenzie, M., Han, C.S., & Ogrodniczuk, J.S. (2015). Prostate cancer support groups: Canada-based specialists’ perspectives. American Journal of Men’s Health, 9, 163–172. https://doi.org/10.1177/1557988314543510
Orom, H., Biddle, C., Underwood, W., III, & Nelson, C.J. (2018). Worse urinary, sexual and bowel function cause emotional distress and vice versa in men treated for prostate cancer. Journal of Urology, 199, 1464–1469. https://doi.org/10.1016/j.juro.2017.12.047
Paterson, C., Robertson, A., Smith, A., & Nabi, G. (2015). Identifying the unmet supportive care needs of men living with and beyond prostate cancer: A systematic review. European Journal of Oncology Nursing, 19, 405–418. https://doi.org/10.1016/j.ejon.2014.12.007
Pawson, R., & Tilley, N. (1997). Realistic evaluation. Thousand Oaks, CA: Sage.
Pollack, L.A., Hawkins, N.A., Peaker, B.L., Buchanan, N., & Risendal, B.C. (2011). Dissemination and translation: A frontier for cancer survivorship research. Cancer Epidemiology, Biomarkers and Prevention, 20, 2093–2098.
Punnen, S., Cowan, J.E., Dunn, L.B., Shumay, D.M., Carroll, P.R., & Cooperberg, M.R. (2013). A longitudinal study of anxiety, depression and distress as predictors of sexual and urinary quality of life in men with prostate cancer. BJU International, 112, E67–E75. https://doi.org/10.1111/bju.12209
Ralph, N., Birks, M., & Chapman, Y. (2015). The methodological dynamism of grounded theory. International Journal of Qualitative Methods, 14, 1609406915611576. https://doi.org/10.1177/1609406915611576
Ralph, N., Chambers, S., Pomery, A., Ollife, J., & Dunn, J. (2019). Nurse-led supportive care intervention for men with advanced prostate cancer. Oncology Nursing Forum, 46, 92–103. https://doi.org/10.1188/19.ONF.92-103
Skolarus, T.A., Wolf, A.M., Erb, N.L., Brooks, D.D., Rivers, B.M., Underwood, W., III, . . . Cowens-Alvarado, R.L. (2014). American Cancer Society prostate cancer survivorship care guidelines. CA: A Cancer Journal for Clinicians, 64, 225–249. https://doi.org/10.3322/caac.21234
Smith, D.P., Supramaniam, R., King, M.T., Ward, J., Berry, M., & Armstrong, B.K. (2007). Age, health, and education determine supportive care needs of men younger than 70 years with prostate cancer. Journal of Clinical Oncology, 25, 2560–2566.
Stacey, D., Légaré, F., Lewis, K., Barry, M.J., Bennett, C.L., Eden, K.B., . . . Trevena, L. (2017). Decision aids for people facing health treatment or screening decisions. Cochrane Database of Systematic Reviews. Retrieved from https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001431.pub5…
Steginga, S.K., Occhipinti, S., Dunn, J., Gardiner, R.A., Heathcote, P., & Yaxley, J. (2001). The supportive care needs of men with prostate cancer (2000). Psycho-Oncology, 10, 66–75. https://doi.org/10.1002/1099-1611(200101/02)10:1<66::AID-PON493>3.0.CO;…
Steginga, S.K., Smith, D.P., Pinnock, C., Metcalfe, R., Gardiner, R.A., & Dunn, J. (2007). Clinicians’ attitudes to prostate cancer peer-support groups. BJU International, 99, 68–71. https://doi.org/10.1111/j.1464-410X.2006.06545.x


